| Size | Price | Stock | Qty |
|---|---|---|---|
| 500mg |
|
||
| Other Sizes |
|
































| ln Vitro |
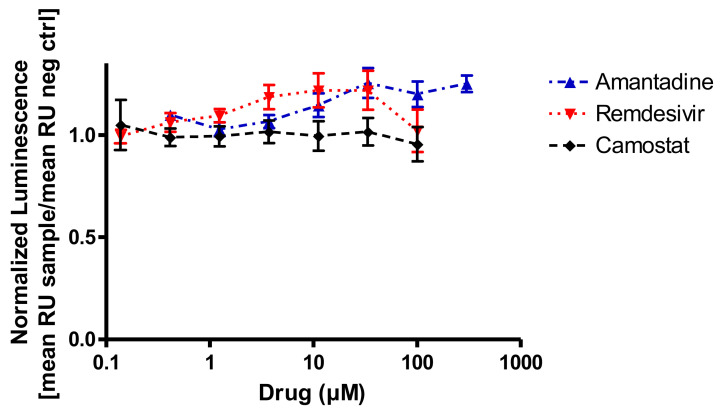
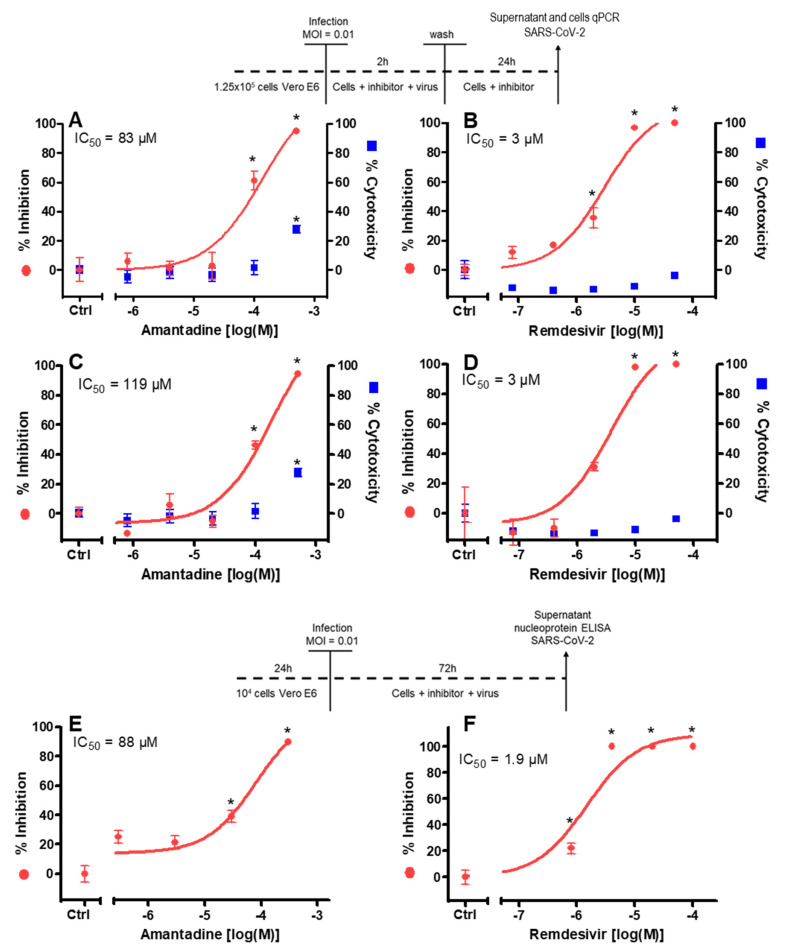
The suppression of SARS-CoV-2 replication by amantadine (0-500 µM, 26 hours) ranges in IC50 values from 83 to 119 µM [4]. Amantadine (0-100 µg/mL, 24-72 hours) strongly suppresses HepG2 and SMMC-7721 cell growth [6]. Amantadine (0-75 µg/mL, 48 hours) causes apoptosis and stops the cell cycle in the G0/G1 phase [6]. Amantadine (0-75 µg/mL, 48 hours) decreases Bcl-2, increases Bax protein and mRNA levels, and decreases cell cycle-related genes and proteins (cyclin D1, cyclin E, and CDK2) [6].
|
|---|---|
| ln Vivo |
Amantadine (25 mg/kg, IP, once day for 3 days) reduces surgery-induced neuroinflammation and learning and memory deficits [5].
|
| Cell Assay |
Cell Viability Assay[4]
Cell Types: Vero E6 Cell Tested Concentrations: 500 µM, 100 µM, 20 µM, 4 µM and 8 nM Incubation Duration: 26 hrs (hours) Experimental Results: Causes concentration-dependent reduction of virus (IC50=83 µM) 26 post-infection The nucleic acid concentration in the supernatant is 10-500 µM. Results in a concentration-dependent reduction of viral nucleic acid in the cytoplasm (IC50=119 µM) 26 hrs (hours) post-infection. Cell proliferation assay[6] Cell Types: Human HCC cell lines (HepG2 and SMMC-7721) and normal liver cells (L02 cells) Tested Concentrations: 0, 1, 2, 5, 10, 25, 50 and 100 µg/mL Incubation Duration: 24, 48 and 72 hrs (hours) Experimental Results: Inhibited cell proliferation in a time- and dose-dependent manner in HepG2 and SMMC-7721 cells. Cell cycle analysis[6] Cell Types: HepG2 and SMMC-7721 Cell Tested Concentrations: 0, 10, 25, 50 and 75 µg/mL Incubation Duration: 48 hrs (hours) Experimental Results: Significant increase in the number of HepG2 and SMMC-7721 cells in G0/G1 phase in a dose-dependent manner, and Dramatically diminished the numbe |
| Animal Protocol |
Animal/Disease Models: Fischer 344 rats (4 months old, male, 290-330 g, 15 rats per group) [5]
Doses: 25 mg/kg Route of Administration: IP, one time/day for 3 days (first dose in 15 minutes before administration) Experimental Results: Inhibited surgery-induced neuroinflammation and learning and memory impairment, increased GDNF (glial cell line-derived neuronal neuron) co-localized with hippocampal glial fibrillary acidic protein (an astrocyte marker) nutritional factors). |
| ADME/Pharmacokinetics |
Absorption, Distribution and Excretion
Amantadine is well absorbed orally from the gastrointestinal tract. It is primarily excreted unchanged in the urine by glomerular filtration and tubular secretion. 3 to 8 L/kg [healthy subjects] 0.2 - 0.3 L/hr/kg 0.10 +/- 0.04 L/hr/kg [healthy, elderly male] Rapidly and almost completely absorbed from gastrointestinal tract. Amantadine is distributed into breast milk. Elimination: Renal; >90% excreted unchanged in urine by glomerular filtration and renal tubular secretion. Rate of excretion rapidly increased in acid urine. In dialysis: Only small amounts (approximately 4%) removed from the blood by hemodialysis. Distributed into saliva, tear film, and nasal secretions; in animals, tissue (especially lung) concentrations are higher than serum concentrations. Crosses the placenta and blood-brain barrier; distributed into breast milk. Cerebral spinal fluid concentrations were 52% of corresponding plasma concentrations in one patient. VolD - 4.4 + or - 0.2 L/kg (normal renal function); 5.1 + or - 0.2 L/kg (renal failure). For more Absorption, Distribution and Excretion (Complete) data for AMANTADINE (7 total), please visit the HSDB record page. Metabolism / Metabolites No appreciable metabolism, although negligible amounts of an acetyl metabolite have been identified. Eight metabolites of amantadine have been identified in human urine. One metabolite, an N-acetylated compound, was quantified in human urine and accounted for 5-15% of the administered dose. Plasma acetylamantadine accounted for up to 80% of the concurrent amantadine plasma concentration in 5 of 12 healthy volunteers following the ingestion of a 200 mg dose of amantadine. Acetylamantadine was not detected in the plasma of the remaining seven volunteers.. No appreciable metabolism, although negligible amounts of an acetyl metabolite have been identified. Amantadine is well absorbed orally from the gastrointestinal tract. The mechanism of its antiparkinsonic effect is not fully understood, but it appears to be releasing dopamine from the nerve endings of the brain cells, together with stimulation of norepinephrine response. The antiviral mechanism seems to be unrelated. The drug interferes with a viral protein, M2 (an ion channel), which is needed for the viral particle to become "uncoated" once it is taken inside the cell by endocytosis. Metabolites are excreted in the urine (A308). Route of Elimination: It is primarily excreted unchanged in the urine by glomerular filtration and tubular secretion. Half Life: Mean half-lives ranged from 10 to 14 hours, however renal function impairment causes a severe increase in half life to 7 to 10 days. Biological Half-Life Mean half-lives ranged from 10 to 14 hours, however renal function impairment causes a severe increase in half life to 7 to 10 days. Amantadine pharmacokinetics were determined in 24 normal adult male volunteers after the oral administration of a single amantadine hydrochloride 100 mg soft gel capsule. ... The half-life was 17 + or - 4 hours (range: 10 to 25 hours). Across other studies, amantadine plasma half-life has averaged 16 + or - 6 hours (range: 9 to 31 hours) in 19 healthy volunteers. Normal renal function: 11 to 15 hours. Elderly patients: 24 to 29 hours. Renal function impairment, severe: 7 to 10 days. Hemodialysis: 24 hours. The elimination half-life increases two to three fold or greater when creatinine clearance is less than 40 mL/min/1.73 sqm and averages eight days in patients on chronic maintenance hemodialysis. |
| Toxicity/Toxicokinetics |
Toxicity Summary
The mechanism of its antiparkinsonic effect is not fully understood, but it appears to be releasing dopamine from the nerve endings of the brain cells, together with stimulation of norepinephrine response. It also has NMDA receptor antagonistic effects. The antiviral mechanism seems to be unrelated. The drug interferes with a viral protein, M2 (an ion channel), which is needed for the viral particle to become "uncoated" once it is taken inside the cell by endocytosis. Hepatotoxicity Despite widespread use, there is little evidence that amantadine when given orally causes liver injury, either in the form of serum enzyme elevations or clinically apparent liver disease. Likelihood score: E (unlikely cause of clinically apparent liver injury). Effects During Pregnancy and Lactation ◉ Summary of Use during Lactation It is probably best to avoid amantadine during breastfeeding because of its potential negative effect on lactation. ◉ Effects in Breastfed Infants Relevant published information was not found as of the revision date. ◉ Effects on Lactation and Breastmilk Amantadine is a dopamine agonist. Clinical studies using amantadine dosages of 100 mg 2 or 3 times daily have demonstrated a decrease in serum prolactin and decreased galactorrhea in patients taking dopaminergic neuroleptic drugs such as phenothiazines, haloperidol and loxapine.[1][2] No studies have been reported on the effects of amantadine on the milk supply in nursing mothers. The maternal prolactin level in a mother with established lactation may not affect her ability to breastfeed. Protein Binding Approximately 67% bound to plasma proteins over a concentration range of 0.1 to 2.0 µg/mL. Toxicity Data LD50: 800 mg/kg (Oral, Rat) LD50: 700 mg/kg (Oral, Mouse) Interactions The anti-influenza A activities of amantadine and ribavirin were investigated seperately and in combination. In ferret tracheal ciliated epithelium, the combination of drugs synergistically delayed the virus-induced cytopathic effect. Concurrent use /of alcohol/ with amantadine is not recommended since this may increase the potential for CNS effects such as dizziness, lightheadedness, orthostatic hypotension, or confusion. Concurrent use /of anticholinergics, or other medications with anticholinergic activity; tricyclic antidepressants; other antidyskinetics; antihistamines; or phenothiazines/ with amantadine may potentiate the anticholinergic-like side effects, especially those of confusion, hallucinations, and nightmares; dosage adjustments of these medications or of amantadine may be necessary; also, patients should be advised to report occurrences of gastrointestinal problems promptly since paralytic ileus may occur with concurrent therapy. Concurrent use /of opioid- and anticholinergic-containing antidiarrheals/ with amantadine may potentiate the anticholinergic-like side effects; although significant interaction is unlikely with usual doses of opioid- and anticholinergic-containing antidiarrheals, significant interaction may occur if these medications are abused. For more Interactions (Complete) data for AMANTADINE (10 total), please visit the HSDB record page. |
| References | |
| Additional Infomation |
Therapeutic Uses
Antiparkinson Agents; Antiviral Agents; Dopamine Agents Amantadine is used in the management of certain aspects of fatigue associated with multiple sclerosis, including lowered energy level, deceased sense of well-being, decreased perceived attention and memory, and diminished problem solving ability. /NOT included in US or Canadian product labeling/ Amantadine is indicated in the treatment of idiopathic parkinsonism (paralysis agitans; shaking palsy), post-encephalitic parkinsonism, drug-induced extrapyramidal reactions, symptomatic parkinsonism following injury to the nervous system caused by carbon monoxide intoxication, and parkinsonism associated with cerebral arteriosclerosis in the elderly. /Included in US product labeling/ Amantadine is indicated as a primary agent in the prophylaxis and treatment of respiratory tract infections caused by influenza A virus strains in high-risk patients (including those with pulmonary or cardiovascular disease, the elderly, and residents of nursing homes and other chronic care facilities who have chronic medical conditions), hospital ward contacts of high-risk patients, immunocompromised patients, those in critical public service positions (eg, police, firefighters, medical personnel), in high-risk patients for whom the influenza vaccine is contraindicated, and patients with severe influenza A viral infections. It is effective against all strains of influenza A virus that have been tested to date, including Russian, Brazilian, Texan, London, and others. It may be given as chemoprophylaxis concurrently with inactivated influenza A virus vaccine until protective antibodies develop. However, it should be emphasized that vaccination of high-risk persons each year is the single most important measure for reducing the impact of influenza. No well-controlled studies have examined whether amantadine prevents complication of influenza A in high-risk persons. Resistant strains of influenza A have been reported in patients receiving rimantadine; these resistant strains were also apparently transmitted household contacts. Rimantadine has a similar chemical structure, spectrum of activity, and mechanism of action to amantadine, and drug-resistant strains of virus have cross-resistance to amantadine and rimantadine. /Included in US product labeling/ For more Therapeutic Uses (Complete) data for AMANTADINE (6 total), please visit the HSDB record page. Drug Warnings Swine influenza (H1N1) viruses contain a unique combination of gene segments that have not been reported previously among swine or human influenza viruses in the US or elsewhere. The H1N1 viruses are resistant to amantadine and rimantadine but not to oseltamivir or zanamivir. Suicide attempts (resulting in death in some patients) have been reported rarely in patients receiving amantadine, many of whom received short courses of the drug for influenza prophylaxis or treatment. The manufacturer states that the incidence and pathophysiology of these suicide attempts are not known. Suicide ideation or attempts have been reported in patients with or without a prior history of psychiatric disorders. Amantadine can exacerbate mental status in patients with a history of psychiatric disorders or substance abuse. Patients with suicidal tendencies may exhibit abnormal mental states including disorientation, confusion, depression, personality changes, agitation, aggressive behavior, hallucinations, paranoia, other psychotic reactions, somnolence, or insomnia. Possible neuroleptic malignant syndrome (NMS) has been reported in patients receiving amantadine and was associated with dosage reduction or withdrawal of the drug. NMS is potentially fatal and requires immediate initiation of intensive symptomatic and supportive care. Patients should be observed closely when the dosage of amantadine is reduced or the drug is discontinued; this precaution is especially important in patients receiving concomitant therapy with an antipsychotic agent. Nausea is one of the most frequent adverse effects of amantadine and has been reported in 5-10% of patients receiving the usual dosage of the drug. Anorexia, constipation, diarrhea, and dry mouth have been reported in 1-5% and vomiting has been reported in up to 1% of patients receiving amantadine. Abdominal discomfort or dysphagia also has been reported. The incidence of adverse GI effects is comparable for amantadine and rimantadine. For more Drug Warnings (Complete) data for AMANTADINE (19 total), please visit the HSDB record page. Pharmacodynamics Amantadine is an antiviral drug which also acts as an antiparkinson agent, for which it is usually combined with L-DOPA when L-DOPA responses decline (probably due to tolerance). It is a derivate of adamantane, like a similar drug rimantadine. The mechanism of action of amantadine in the treatment of Parkinson's disease and drug-induced extrapyramidal reactions is not known. It has been shown to cause an increase in dopamine release in the animal brain, and does not possess anticholinergic activity. |
| Molecular Formula |
C10H17N
|
|---|---|
| Molecular Weight |
151.2487
|
| Exact Mass |
151.136
|
| CAS # |
768-94-5
|
| Related CAS # |
Amantadine hydrochloride;665-66-7;Amantadine-d15;33830-10-3;Amantadine sulfate;31377-23-8;Amantadine-d6;1219805-53-4
|
| PubChem CID |
2130
|
| Appearance |
White to off-white solid powder
|
| Density |
1.1±0.1 g/cm3
|
| Boiling Point |
225.7±8.0 °C at 760 mmHg
|
| Melting Point |
206-208 °C(lit.)
|
| Flash Point |
96.0±9.7 °C
|
| Vapour Pressure |
0.1±0.4 mmHg at 25°C
|
| Index of Refraction |
1.558
|
| LogP |
2.22
|
| Hydrogen Bond Donor Count |
1
|
| Hydrogen Bond Acceptor Count |
1
|
| Rotatable Bond Count |
0
|
| Heavy Atom Count |
11
|
| Complexity |
144
|
| Defined Atom Stereocenter Count |
0
|
| InChi Key |
DKNWSYNQZKUICI-UHFFFAOYSA-N
|
| InChi Code |
InChI=1S/C10H17N/c11-10-4-7-1-8(5-10)3-9(2-7)6-10/h7-9H,1-6,11H2
|
| Chemical Name |
adamantan-1-amine
|
| HS Tariff Code |
2934.99.9001
|
| Storage |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month Note: This product requires protection from light (avoid light exposure) during transportation and storage. |
| Shipping Condition |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| Solubility (In Vitro) |
DMSO : ~10 mg/mL (~66.12 mM)
|
|---|---|
| Solubility (In Vivo) |
Solubility in Formulation 1: ≥ 1 mg/mL (6.61 mM) (saturation unknown) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (add these co-solvents sequentially from left to right, and one by one), clear solution.
For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 10.0 mg/mL clear DMSO stock solution to 400 μL of PEG300 and mix evenly; then add 50 μL of Tween-80 to the above solution and mix evenly; then add 450 μL of normal saline to adjust the volume to 1 mL. Preparation of saline: Dissolve 0.9 g of sodium chloride in 100 mL ddH₂ O to obtain a clear solution. Solubility in Formulation 2: ≥ 1 mg/mL (6.61 mM) (saturation unknown) in 10% DMSO + 90% (20% SBE-β-CD in Saline) (add these co-solvents sequentially from left to right, and one by one), clear solution. For example, if 1 mL of working solution is to be prepared, you can add 100 μL of 10.0 mg/mL clear DMSO stock solution to 900 μL of 20% SBE-β-CD physiological saline solution and mix evenly. Preparation of 20% SBE-β-CD in Saline (4°C,1 week): Dissolve 2 g SBE-β-CD in 10 mL saline to obtain a clear solution. View More
Solubility in Formulation 3: ≥ 0.5 mg/mL (3.31 mM) (saturation unknown) in 10% DMSO + 90% Corn Oil (add these co-solvents sequentially from left to right, and one by one), clear solution. |
| Preparing Stock Solutions | 1 mg | 5 mg | 10 mg | |
| 1 mM | 6.6116 mL | 33.0579 mL | 66.1157 mL | |
| 5 mM | 1.3223 mL | 6.6116 mL | 13.2231 mL | |
| 10 mM | 0.6612 mL | 3.3058 mL | 6.6116 mL |
*Note: Please select an appropriate solvent for the preparation of stock solution based on your experiment needs. For most products, DMSO can be used for preparing stock solutions (e.g. 5 mM, 10 mM, or 20 mM concentration); some products with high aqueous solubility may be dissolved in water directly. Solubility information is available at the above Solubility Data section. Once the stock solution is prepared, aliquot it to routine usage volumes and store at -20°C or -80°C. Avoid repeated freeze and thaw cycles.
Calculation results
Working concentration: mg/mL;
Method for preparing DMSO stock solution: mg drug pre-dissolved in μL DMSO (stock solution concentration mg/mL). Please contact us first if the concentration exceeds the DMSO solubility of the batch of drug.
Method for preparing in vivo formulation::Take μL DMSO stock solution, next add μL PEG300, mix and clarify, next addμL Tween 80, mix and clarify, next add μL ddH2O,mix and clarify.
(1) Please be sure that the solution is clear before the addition of next solvent. Dissolution methods like vortex, ultrasound or warming and heat may be used to aid dissolving.
(2) Be sure to add the solvent(s) in order.
| NCT Number | Recruitment | interventions | Conditions | Sponsor/Collaborators | Start Date | Phases |
| NCT06443827 | Active, not recruiting | Drug: Amantadine Sulfate | Amantadine Consciousness Disorders Electroencephalography |
Azienda Sanitaria dell'Alto Adige | 2018-09-15 | Phase 2 |
| NCT04387773 | Completed | Drug: GOCOVRI | Parkinson Disease | Oregon Health and Science University | 2020-11-05 | Phase 4 |
| NCT03612921 | Unknown status | Drug: oral Amantadine sulfate Drug: i.v Amantadine Sulfate Drug: placebo tablet |
Intubation, Intratracheal | Assiut University | 2018-08-15 | Phase 2 |
| NCT03988010 | Unknown status | Drug: Amantadine Sulfate Drug: Placebo (for amantadine sulphate) |
Postoperative Cognitive Dysfunction | TC Erciyes University | 2019-05-01 | Phase 4 |
| NCT04273737 | Terminated | Drug: Amantadine Hydrochloride | Cerebral Palsy | Columbia University | 2020-02-28 | Phase 4 |
|
|
Products are for research use only; We do not sell to patients
Copyright 2020 InvivoChem LLC | All Rights Reserved